
Vaccines, Sophistry, and Immunobridging!!
Vaccines, Sophistry, and Immunobridging!!
Immunobridging!! of studies proves some very interesting stuff that should be considered in all future VRBPAC meetings.

Do you think that the definition of vaccination is “the act of introducing a vaccine into the body to produce immunity to a specific disease?” It is the definition of vaccination that almost every healthcare provider used in our professional formation. It also is the definition that our patients still mean when they use the term. If it was Before Covid, you would be correct.
March 2020 Way Back Machine of CDC Definition of Terms:
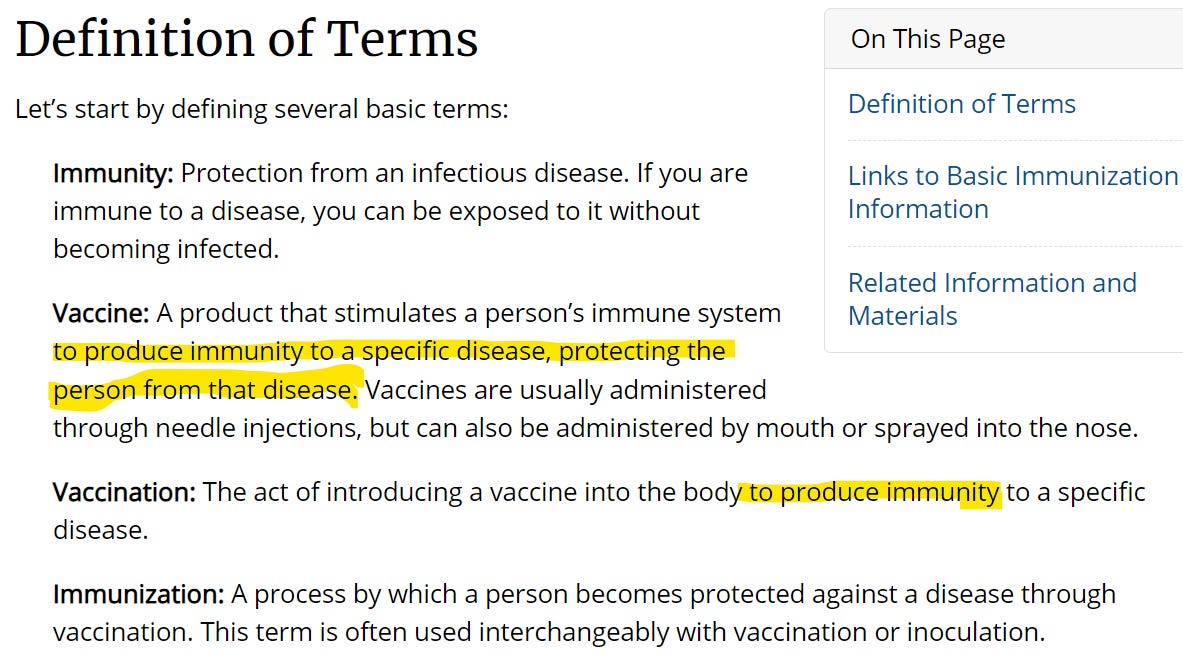
At some point the definition changed, so that today the same CDC page defines the terms differently:
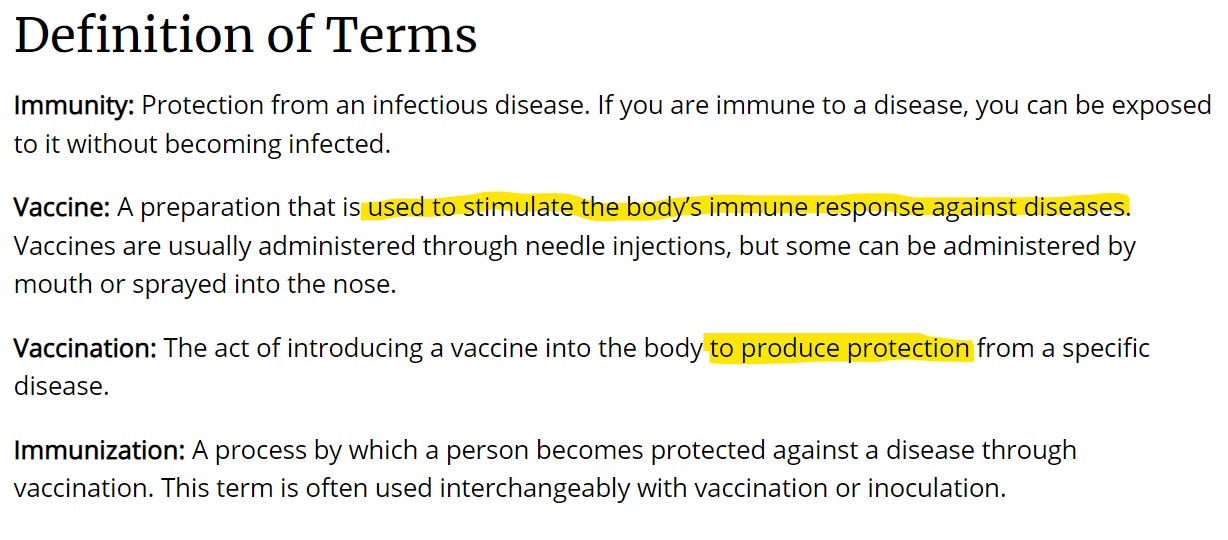
The change from immunity to “stimulate the bodies immune response” is extremely important if we are going to understand the FDA Vaccines and Related Biological Products Advisory Committee meetings in regards to Products that are sold to the US Government as Counter Measures under the PREP Act against COVID19.
With this sophistry, the CDC has changed the regulatory approval process for vaccines to no longer need to focus on efficacy of the products on human beings in the real world at preventing people from getting sick and spreading diseases, but on test subject’s laboratory confirmed immune responses which are then assumed to corelate to real world data.
The ability of these products to induce someone to make antibodies are now what matters when one discusses Vaccines in a FDA VRBPAC committee, much more so than actual proof that the Vaccines produce immunity.
What about Boosters?
If antibodies are made, and the antibodies at specific concentrations can neutralize virus in Petri dishes (in practice other laboratory tests are used) then the deduction is that the Products are Effective, and should be approved.
While there are a few BIG problems with this paradigm, one is that the virus in the real world is undergoing evolutionary pressures. The virus doesn’t play by laboratory rules when it is in the real world. As with all coronaviruses the virus responsible for COVID19, SARSCOV2, is changing rapidly in the real world and always seeking out the best fit to replicate itself and spread. The mRNA in Moderna and Pfizer products and coded proteins in Novavax DO NOT code a tight match to the current virus circulating today, which is predominantly different strains of Omicron. They all code for a Laboratory modified version of the Original Wild Type Spike Protein from 2019/Jan 2020.
True to Science based on Sophistry, Boosters so far have all been designed to increase a persons immune response against the original target protein (an adaption of the wild type Spike Protein). The rationale is as follows: Usually antibodies need to have a very tight fit to work well, but even if there is a bad fit to an antigen (like the case with Omicron spike vs products based on Wild type spike with lab adjustments) if the antibody concentration is high enough, it will still be able to neutralize the virus in a laboratory model in which the virus does not then respond and adapt.
How are boosters approved for COVID19 genetic product preventative Countermeasures in 2022? BAD Pharma has to show that the booster injections can mount even higher antibody levels that can then in higher concentrations neutralize virus that is not a tight fit for those antibodies. The science has only showed that the products can induce immune responses that are able to neutralize virus in a laboratory.
Now comes Immunobridging!!
(Let’s try a new rule: Because ImmunoBridging!! is a ridiculous concept, to properly discuss it, we should incorporate a little bit of ridiculousness. Therefore when you read Immunobridging!! Please Imagine it is being yelled loud without any inflection.)
, What is Immunobridging!! anyway? Don't take my word for it:
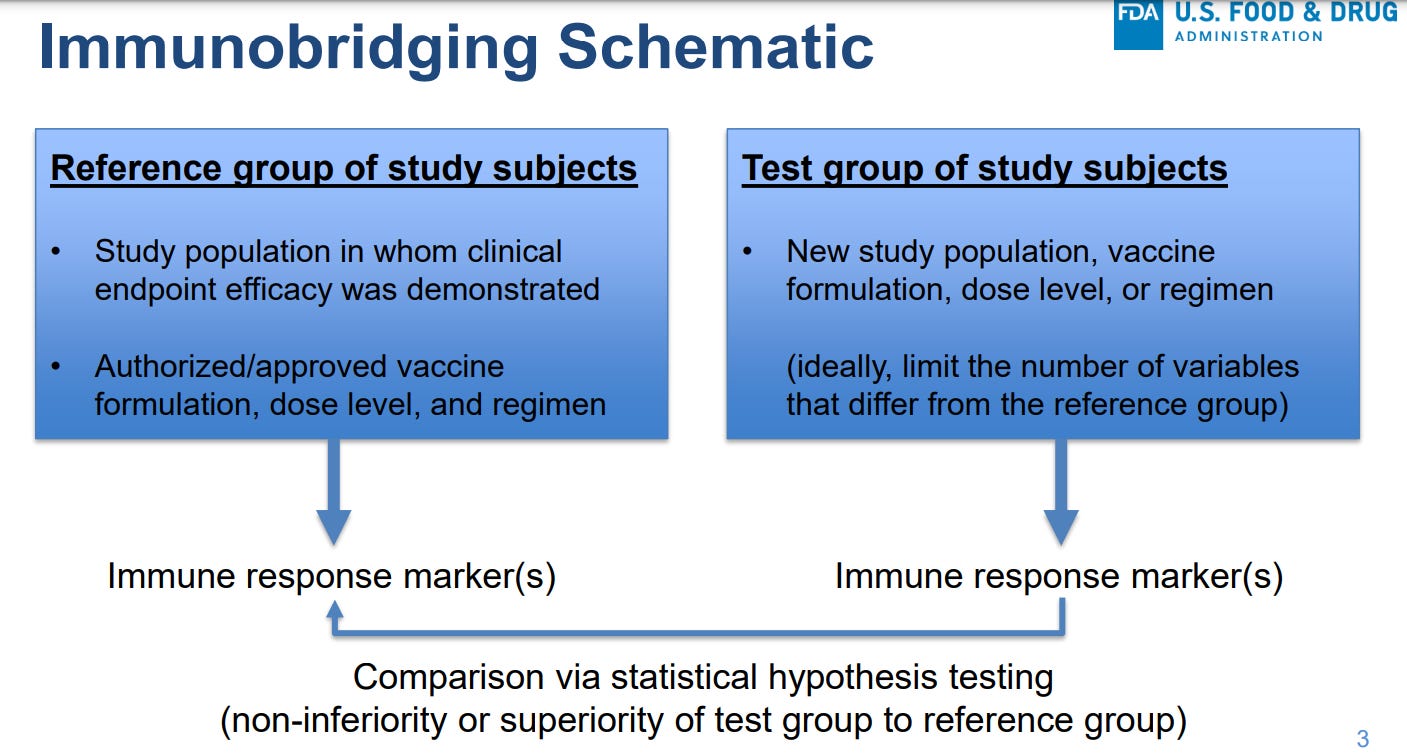
Since immune response matters, antibodies or ‘immune response markers’ are how we determine Immunobridging!!
We measure antibody concentrations in a group of test subjects that are 6month old through 17 years old, and cross-reference to antibody concentrations in another population of test subjects in the 18-25 year old population. Then because the genetic products have been approved in the 18-25 year old for the immune response that is made in that population, FDA and other Government Regulatory agencies around the world should justify Emergency Use Authorization of the products for infants , toddlers and children. I am going to break this down for you.
Remember the Transitive Property of Equality?
if A=B and A=C then B=C
That’s Immunobridging!! in a nutshell.
A= Antibodies for Adults
B= Efficacy Study results, adults and Approval of Product
C= Antibodies for Babies and Children
A =B
Antibody levels for adults= Efficacy Study results Adults and Approval of Product
A = C
Antibody levels for adults= Antibody levels for babies and Children
IMMUNOBRIDGING!!
C=B
Antibody levels for babies and children =Study Result Adults and Approval of Product
Immunobridging!! is what the studies on children were primarily designed to investigate and why the products were approved unanimously at the FDA VRBPAC and ACIP CDC meetings 2 weeks ago.
Now you know.

But are children little adults? Should the Transitive property of Equality even be used in this way? Ask any healthcare provider the following question:
Do Immune systems of babies and children behave equally to immune systems of adults and seniors?
I will summarize it as: Immunobridging!! rests on an understanding of Human Development that equates human immune system responses across ages of populations. Thymic Development be Damned!
(For my non medical readers: as it turns out Thymic Development matters a whole lot in human Immune systems, and it is not equal across age populations).
Let’s leave further discussions of this to another day.
However, if Immunobridging!! is worth something, like the WHO, FDA, and CDC seem to believe, one should draw some very concerning conclusions from the Materials of the June 14th and 15th FDA VRBPAC meeting. The Transitive Property of Equality works BOTH ways.
SO… there’s a new data point now and that is how well the antibodies predict efficacy in the real world against Omicron, and how safe the Vaccines are for 6 month through 4-5 year olds. If antibodies in babies equates to studies in adults, then studies in babies must equate to antibodies in adults.
Did you get that?
Study Results for Babies=D
C=D
Antibody levels for babies and Children= Study Results for Babies and Children
IMMUNOBRIDGING!!
D=A
Study Results for babies and children = Antibody levels of Adults.
So in a worldview where
Antibodies are the thing that a vaccine needs to make,
Antibody levels can through Immunobridging!! demonstrate vaccine equality for all age groups in order to show that
Approvals for a vaccine must apply to another age group,
Because the COVID19 is changing,
The studies of the most recent age group MUST be used to determine how well the product actually works for ALL the populations to which Immunobridging!! has been demonstrated.
Safety signals associated with any of the studies must also be considered by ALL of the equated populations.
And let’s look again at the data that was presented to the FDA VRBPAC by Pfizer and Moderna on their recent studies. It is summarized very well by James Roguski:
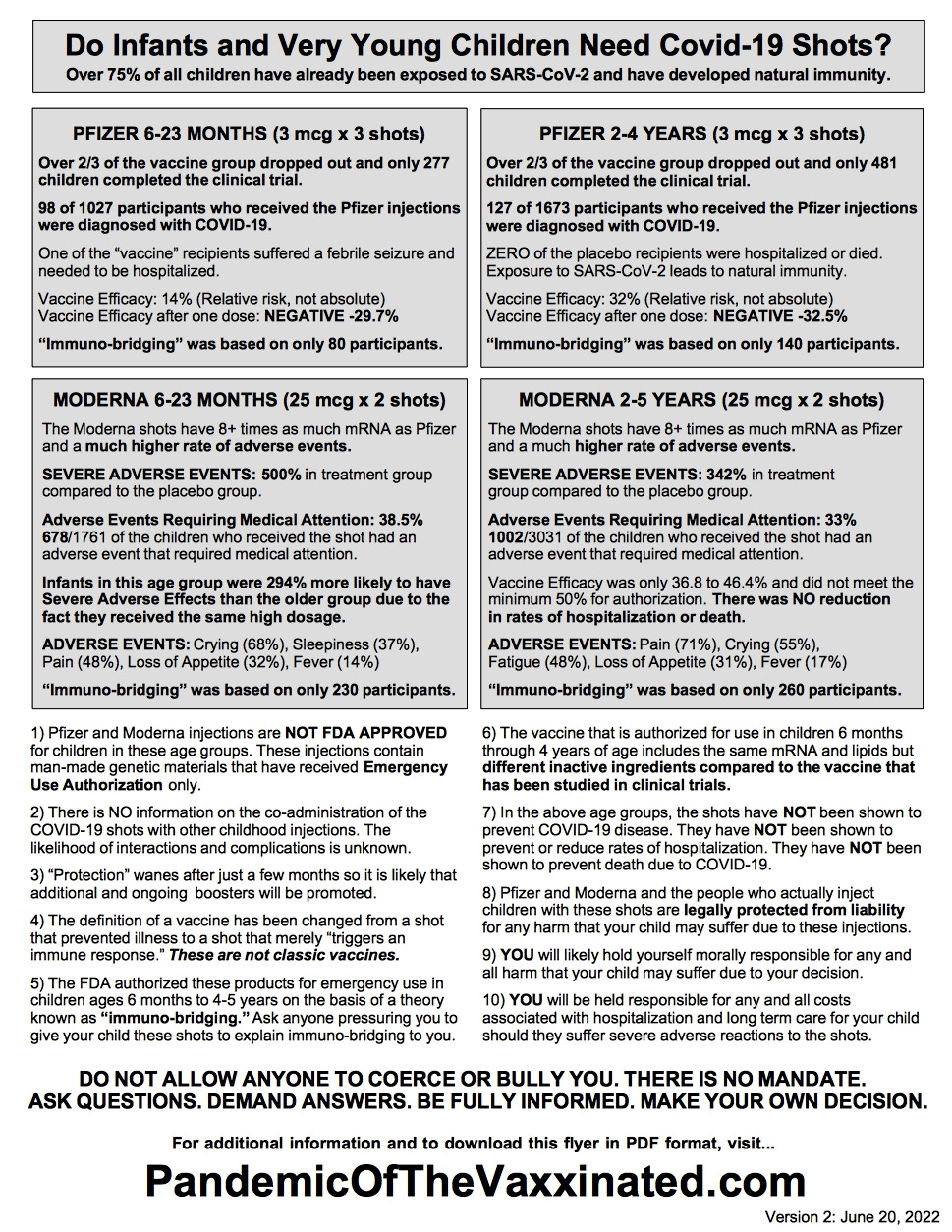
Because of Immunobridging!!, Pfizer and Moderna each did a study that demonstrated that all of their vaccines cause harm and are ineffective in the real world.
But if that were the case wouldn’t we have seen the increased adverse events in the original data?
In fact we did, but it wasn’t discussed or evaluated by BAD Pharma or the FDA, CDC, or WHO.
Check out this substack by Dr. Malone in which he discusses the recent paper that analyzes the original phase 3 trials by Moderna and Pfizer, and finds similar trend of increased rates of serious adverse events in the original phase 3 Moderna and Pfizer studies that are seen in the recent pediatric studies.
Dr. Peter Doshi is the senior author of the paper that is reanalyzing the Moderna and Pfizer Vaccines as Dangerous, in their own Studies that were given to the FDA. Dr. Doshi is not a fringe anti-science person. Dr. Doshi is the Senior Editor of the British Medical Journal. He is not analyzing NEW data. They knew this all along.
One more time for the inter-web censors and record keepers:
Dr. Peter Doshi, the Senior Editor of the British Medical Journal, is Senior author of a paper that analyzes the original Moderna and Pfizer Phase 3 trials from 2020 and finds very concerning trend of increased serious adverse effects in the arms that received the experimental genetic products…
and the FDA, CDC, Pfizer, and Moderna are refusing to release the data at a detailed level that is necessary for a more complete analysis.
I wonder why? Anybody have a guess?
So what is the next step?
Secretly to all the Censorship police and the Professional Association Inquisitors in the AMA (check out my substack on that here) but in plain site to us all on June 28th the FDA meeting is about the NOT EFFECTIVE side of the equation, and ignoring the whole inconvenient “it’s Harmful” thing. So the questions posed to the committee are having to do with “to what extent should the FDA further do away with science in the authorization and approval process for changes in Ineffective Genetic Products.”
Instead of following the Science, which would also include the HARMFUL part of the equation, the FDA has found science to be too difficult for BAD Pharma and so with the CDC and the WHO they have decided instead to be sneaky regulatory sophists and redefine words and adjust the protocols in order to justify continuing massive genetic product programs that have been proven by the Sponsors to be harmful and all agree ineffective.
They released the meeting briefing here. For more check out James Roguski’s Substack on it:

If you haven’t made public comment yet, I encourage you to. You have until 11:59pm ET on Monday June 27th. Thanks to James for his work on this. He has links to both in his website above.
Thanks for Subscribing to Stranger and Sojourner and thanks for the Shares!
Thank you Anthony! The pediatric practice I work for is giving these vaccines to babies now :-(